Special Edition: Nottingham Maternity Review

By: Lauren Monaghan, LDRS
Undignified body storage, an early gestational baby being disposed of as clinical waste and 156 babies who could have survived under better care.
These are just some of the harrowing maternity realities thousands of mothers, babies and families have had to endure under the care of Nottingham hospitals.
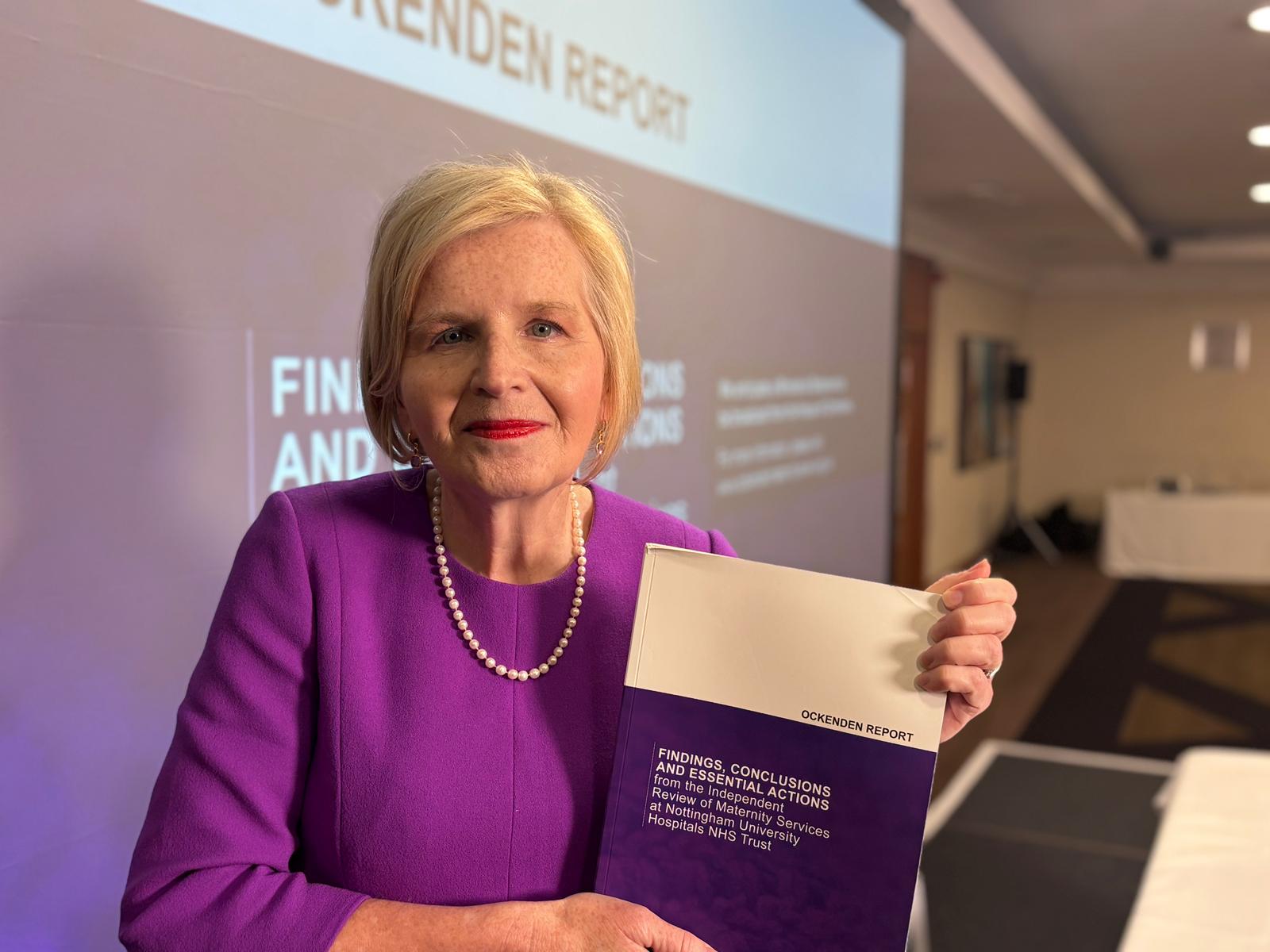
For nearly four years, Donna Ockenden’s independent maternity review has been unravelling care failings under Nottingham University Hospitals Trust’s (NUH) maternity and neonatal services as far back as 2006, though the majority of cases are from 2012.
Examining 2,505 cases of death and serious harm, and involving 2,430 families and 822 staff, the review is the largest in NHS history.
On Wednesday (June 24), distressing details of the report were read out by Ms Ockenden to an audience of impacted families and the media while on a live broadcast.
Of the 2,505 cases, 612 relate to severe maternal harm, 505 relate to stillbirths, 329 relate to neonatal deaths – within the first 28 days of life – 297 relate to brain injuries at birth, 24 relate to maternal deaths and 535 relate to additional maternity experiences.

One stark outcome from the review is that it found 156 babies could have survived had better care been provided by NUH over a period of 13 years, relating to 94 stillbirths and 62 neonatal deaths.
There were also 105 potentially avoidable severe brain injuries inflicted on babies.
Devastating details around the handling of babies and a mother after death have also been revealed.
In 2016, after death, one baby was placed by a member of the portering staff into a mortuary space already occupied by an unrelated deceased adult patient – the parents were not notified of this until 2026.
Later in 2019, a very early gestational baby was “inadvertently” disposed of as clinical waste, with Ms Ockenden calling this a “complete loss of dignity” and said it caused “significant distress” for the parents.
The report details the case of a mother who died in 2021 and was allowed to deteriorate so much in the hospital mortuary that her mother was not able to view her body.
Speaking to the families and media, Ms Ockenden said: “What emerges from those testimonies, consistently and painfully, across more than a decade, is a pattern of families not being listened to, not being believed and being dismissed or minimised.
“Women who raised concerns about their baby’s movement, or their baby’s lack of growth, being told they were anxious and imagining it.”
She continued that women were repeatedly “turned away” after multiple calls for help during labour and denied C-sections.
Reacting to the published report, Sarah Hawkins, whose daughter Harriet was stillborn at Nottingham City Hospital in 2016, said:
“It was really difficult, because it should never have happened.
“So much was preventable. Had they listened to us in 2016 or had they listened to people before us, there’d be no one in that room today.”
Jack Hawkins, Harriet’s dad, said:
“The normalisation of harm in maternity is extraordinary.
“We’re buoyed by the strength of the findings and the strength of Donna’s delivery.
“There is no reason that the immediate and essential actions from this report can’t be made mandatory today – there’s no reason at all.”
The families involved in the review are calling for a national public inquiry into maternity failings – a judge-led investigation which compels witnesses to give evidence on an issue.
Mr Hawkins says he has “zero faith” that changes to maternity services will happen unless a statutory public inquiry happens.
He said:
“We’ve had Morecambe Bay [investigation], Shrewsbury and Telford [review], we’ve had Nottingham – none of them are saying vastly different things.
“Until we understand why maternity is unsafe in this country through a statutory public inquiry, I have no expectation that things will be better.”
Felicity Benyon, who had her bladder accidentally removed during a C-section at Queens Medical Centre in 2015 said it was “heartbreaking” to hear the numbers of impacted babies and mothers in the review, and how many “should still be here”.
She said:
“The preventable bit is the hardest bit. When anything happens to you it’s hard to deal with how that massively changes your life.
“But when you know it should never had happened, if people had done their job properly, you wouldn’t be living with the lifelong harm and trauma that comes with that, it’s a whole other level of pain.”
Speaking on the calls for a public inquiry, Ms Benyon said:
“We need to know was it certain consultants, certain midwives, that instigated ways of working and poor culture, poor lack of accountability which has then crept up as they’ve got promotions, or whether it’s come from the top down.”
“This [review] has taken that pain and tried to turn it into a little positive, trying to focus that on not wanting anyone else to go through what I’ve gone through… we’re not stopping, this is not the end.”
Anthony May, chief executive of NUH, said he was “extremely sad” over the review’s findings, but said he had admiration for the courage the families had shown through the process and “determined” to build on the trust’s maternity improvements.
He said:
“We have been open and transparent about our failures from day one… we’ve tried to be humble, and see things from their [families] point of view and we’ve grafted really hard to try and improve the services.”
Mr May said that when he joined the trust in 2022, NUH hit five out of the 10 safety recommendations in maternity, but it now meets all 10. It also had around 126 vacancies for midwives at the time which is now down to 15.

He said:
“We owe it now to these families and we owe it to local women to rebuild trust and make things better.
“It means something to me because I live here, it’s my hospital, it’s been a privilege to get to know those really courageous families and learn from them.”
Speaking on the review’s alarming mortuary findings, Mr May said:
“It’s very disappointing… it’s a horrendous thing and I’m so sorry about that, it should have never have happened – we did not protect the dignity and respect of those families.
“We also commissioned a separate review into mortuary services today… I’m personally determined to fix it, I feel very disappointed personally that it’s happened on my watch.”
Other key concerns outlined by Ms Ockenden include:
- Multiple factors contributed to harm: “Harm was rarely the result of a single issue or specific failing. Adverse outcomes were linked to multiple interacting factors, this included communication failures, delayed escalation, inadequate risk assessment and governance weaknesses.”
- Staffing pressures left services operating in “crisis mode”: “Chronic staffing shortages and operational pressures significantly impacted both the quality of care and staff wellbeing. Many staff reported working in sustained ‘crisis mode’, with concerns raised repeatedly without sufficient resolution.”
- A poor workplace culture prevented staff from speaking up: “The Review Team has found multiple serious issues with workplace culture within the Trust, including bullying, hierarchy and poor psychological safety, which affected decision-making and prevented members of staff from voicing their concerns. This had direct implications for patient safety.”
- Inequalities in care contributed to poor experience and outcomes: “The Review Team identified that inequalities affect both experiences and outcomes. Women from Black, Asian and other ethnic minority backgrounds, as well as those experiencing deprivation or social vulnerability, often faced additional challenges in accessing safe or personalised care.”
- Key maternity events not being escalated to the trust’s board at the time they happened: including the death of Harriet Hawkins and a letter signed by 50 maternity staff expressing safety concerns in 2018, along with “conflicting recollections” of whether issues were known by the board. “At best this points to a culture of denial, at worst one of a cover up” the report says.
Dozens of current and former senior figures across NUH and the wider local NHS were contacted for the review but the engagement was described as “extremely disappointing”.
Only 35 of the 66 NUH senior staff were interviewed despite multiple staff being contacted several times, and only four of 14 senior staff were interviewed from the wider NHS.
Eight “immediate” and “essential” actions in the following areas which “must happen” to improve maternity services at NUH are:
- Improvements in listening to women and families
- Workforce planning and safe staffing
- Training and multi-professional learning
- Risk assessment throughout pregnancy
- Incident investigation and family involvement
- Governance and board accountability
- Culture, teamwork and psychological safety
- Mothers who have died and post death care